

For today’s article, I had the honour of asking Karen Ward her perspective on a number of topics. Karen is a Vancouver-based drug policy artist and advocate. You should follow Karen on Twitter at @kwardvancouver and check out some of her publications like “Name Change Frame Change”.
First, you know how we say “structural power”? Drug prohibition is like a cornerstone of that structure. It holds the whole thing up. It’s used to maintain the carceral state, colonial violence, racial capitalism: establishment of the ruling class of this settler state" (Karen Ward).
August 31st, 2023 is International Overdose Awareness Day (IOAD). Between today (July 29, 2023) and August 31st, at least 198 more British Columbians will die from drug poisonings. Leading up to this day, it is important to share with the public and those in power exactly what is at stake.
In BC, we are entering into the eighth year of the prolonged public health emergency of unregulated drug poisonings. In fact, today marks day 2,662 since an emergency was declared. The impacts of this crisis are far-reaching, carving out an entire generation before our eyes. Our collective grief is immeasurable. Drug poisonings are now the leading cause of death among British Columbians aged 10-59. We call them drug poisonings, instead of overdose, because the unregulated drug supply offers no predictability or quality control. This supply is volatile, consisting of varying concentrations of fentanyl, fentanyl analogues, benzodiazepines, and other non-opioid sedatives. The synergism of these adulterants makes for a deadly concoction.
A policy regression is underway in this province. Calls from people with lived/living experience of drug use, public health experts, and trusted public institutions like BC Coroners Service to address this emergency at the source (by replacing the unregulated drug supply with a regulated safe supply), are going unheeded. Access to prescribed safer supply is on the decline, even while the evidence supporting this practice grows daily. Those who are able to access prescribed safer supply are often offered drugs that do not meet their needs, and in service delivery models that are rife with barriers to accessibility. Prescribed safer supply was never enough on its own, but it did represent an entry point to more meaningful policy reform.

Instead, the anti-safe supply movement has weaponized “just say no” rhetoric to position prescribed safer supply as part of the problem. Hydromorphone, the drug primarily used in BC’s provincial Risk Mitigation Guidance, has been touted as the cause for more harm, despite BC Coroners reporting “there is no indication that prescribed safer supply is contributing to unregualted drug deaths”. A recent report from the BCCDC showed that “the rate of new OUD [opioid use disoder] diagnoses has been stable or declining across all age groups since 2017”.
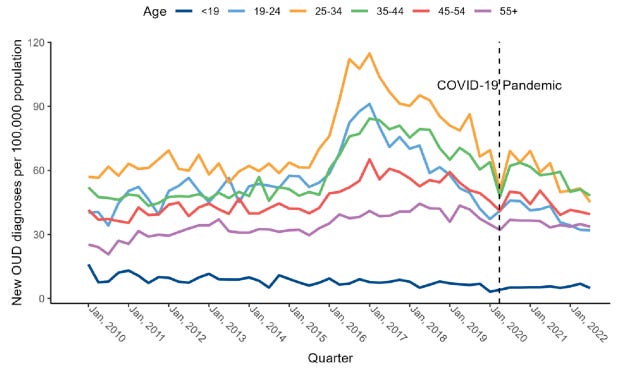
What’s even more important to clarify is that hydromorphone prescribing is very common in BC, and has been well-before prescribed safer supply was implemented. In fact, about 84% of hydromorphone prescribing is for non-safe supply purposes (e.g. management of chronic pain). Most (~94%) of prescribed safer supply recipients are required to pick up their medications daily, whereas those who are not stigmatized with labels like opioid use disorder, are allowed to take mutlitple days and weeks worth of supply home with them. The goal here isn’t to downplay the potential impacts of diversion, but to have open and honest conversations about what is and is not working right now. What we are doing right now, particularly with RMG, is not safe supply. The fixation on hydromorphone, both from advocates and detractors of prescribed safer supply, is problematic. The secret ingredient to addressing the unregulated drug poisoning emergency is options, and no single approach will stop the deaths alone. We should be learning from this experience and innovating new models to effectively replace the unregulated drug supply. Instead, we’ve stagnated, something Karen calls intentional policy failure: “The purpose is to give the appearance of meaningful policy change, not the thing itself.”
https://twitter.com/BerniePauly/status/1666072322938400770?s=20
Prescribed safer supply, at its peak, was reaching around 5% of British Columbians who would qualify for an opioid use disorder diagnosis. This intervention will never reach people who use their drugs episodically, recreationally, or first-time users, all of whom represent the highest risk for fatal drug poisonings because they have no established tolerance. It won’t reach them, because current medicalized models are not designed to meet the needs of the majority at risk. It’s the weekend warrior who dies when he does a bump of coke laced with fentanyl, or the person buying Xanax online and instead getting pill-pressed fentanyl, or the construction worker buying oxys on the block and getting a deadly mix of fentanyl and bromazolam. Prescribed safer supply has a place on the continuum of supports needed to address this emergency, but the false binary of “prescribed safer supply or bust” is causing harm. Until we replace the entire unregulated drug supply, more of our friends, family, and community members will die.
The regression in harm reduction extends beyond the fate of prescribed safer supply. BC’s novel and poorly implemented decriminalization plan is under fire before it’s even six months old. Yes, it’s only been 179 days of a half-measured decriminalization, and political leaders are itching to declare it an abject failure. Municipal bylaws banning public drug consumption are setting their sights on people who have nowhere to go. Given the rise in public vitriol towards the unhoused, it feels intentional that BC’s decriminalization has enabled municipalities to displace and disproportionately target British Columbians who are forced to use their drugs in public settings due to a lack of accessible shelters, overdose prevention services, and housing. This is called structural violence.
Closing the Yaletown overdose prevention service (OPS) is just the latest act of state violence we’ve seen, and another chapter in the BC harm reduction backslide. These are life-saving, evidence-based essential services. All while 2023 poses the potential to be another record-breaking year for drug poisoning deaths. On our way to year eight of this public health emergency, BC is tracking to exceed 2,500 deaths for the first time ever. Closing life-saving services amidst such carnage is an act of social murder.
This is an open call for courage among our elected leaders, municipal and provincial. The answer is not to punish those who are dying on our streets, in shelters, and in their homes. The answer has never been to take away services, but rather continue towards a fully realized continuum of options that are evidence-based and non-coercive. You cannot succumb to divisiveness. You cannot sell your souls for the next election cycle.
Ending drug prohibition is a necessary and irrevocable step to building a better world. This isn’t about drugs. It’s about pulling this structure down. (From Karen Ward’s article Forever Emergencies)
This is a plea for help directed to all British Columbians. We must respond to this emergency with compassion and urgency. The hatred directed towards people who use drugs is misplaced. If visible poverty makes you uncomfortable then advocate for accessible housing. If you do not want to see public drug use, then advocate for safer use spaces. If you do not want to hear about more preventable drug poisoning deaths, then tell your MLA that we must replace the unregulated drug supply with regulated drugs accessible to all. International Overdose Awareness Day is in 33 days. This day is an opportunity to remember those who have been taken from us because of unjust and toxic drug policy. It is also a day to show our strength in solidarity, and to say no to regressive and reactive public policy. The alternative is more death, more loss, more grief.